
Revolutionizing laparoscopic surgeries by targeting 70% of all major complications
>65%
of General surgeries are performed laparoscopically or robotically.

What They Have in Common
- In robotic and laparoscopic surgeries, the surgeon would make several small incisions to insert a camera and surgical devices, as opposed to open surgeries, which involve making one, large opening in the abdomen to operate.
- In order to insert the necessary instruments, javelin-like instruments, called trocars, are used to penetrate the abdominal wall, and serve as portals into the abdomen.
- While laparoscopic and robotic surgeries reduce post-operative pain, recovery time, and other minor complications, the rate of major complications remains the same.

The Problem:
1.Organ and vessel puncture upon trocar insertion
2.Movement of trocar during procedure
3.Poor tissue alignment during wound site closure can lead to later development of hernias
Insertion

- During insertion, the surgeon pushes the trocar in through the abdominal wall.
- Because of the resistive force of the abdominal wall, the surgeon has to push with a great amount of force.
- The moment the trocar is pushed past the last layer of the abdominal wall, it accelerates into the abdomen.
- As the abdominal organs and vessels are at a close proximity to the abdominal wall, this acceleration can cause organ or vessel puncture.
- The average settlement for such complications is $242,000
- No device on the market has successfully solved this problem
Stabilization
- As instruments are being pushed in and out of the abdomen through the trocar, the trocar can slip further in or out of the abdomen than needed.
- No device on the market allows for trocar stabilization.
Closure
- After making several incisions in the abdomen, surgeons should ensure that these incisions were properly closed to prevent herniation.
- As there are several layers in the abdominal wall, it is essential to ensure full-thickness or near full-thickness closure to make sure the holes are properly sealed.
- After the removal of thee trocar, it becomes difficult to reach and separate the bottom layers to ensure optimal closure.
- Improper closure could require subsequent surgeries to repair resulting hernias.

OUR SOLUTION:
- The SafeT device solves all 3 pain ponts.
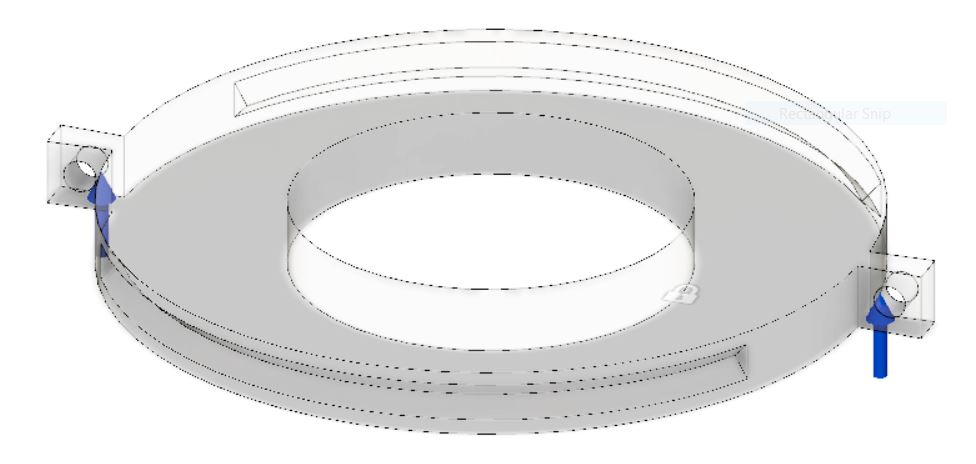
- The first component of the SafeT device (shown in blue) consists of a base, an adhesive that attaches to the skin of the abdominal wall (outside layer), and hooks to which clamps can be attached. This device is used to pull the abdominal wall away from the abdominal organs and add a resistive force during the insertion of the trocar.
- Once the trocar is safely inserted, the second component (shown in red) clamps onto and around the trocar. The inside portion of the component includes ridges to keep the trocar from slipping in and out of the abdomen. The bottom portion of this component is made of flexible material to ensure the flexibility needed when using the trocar.
- The last component is the holes in the red component. The holes are positioned at the right depth and angle to help guide surgeons across all layers of the abdominal wall to ensure full-thickness closure.
Design Requirements
After spending a total of more than 300 hours in the Operation Room, shadowing surgeons as they perform laparoscopic and robotic surgeries, and asking them about their concerns about current devices and qualities they like to see in potential solutions, we have come up with the design requirements and specifications shown in the table below. For some specifications, we designed mock models for surgeons to test on to ensure that the specifications reflect the actual forces as accurately as possible.
| Design Requirement | Specification |
| Durable device | Must withstand >25 lb pulling force |
| Durable adhesive | Must withstand >25 lb tension |
| Flexible | Allow for 2 degrees of freedom (rotation in the transverse and sagittal planes) |
| Angle of needle guide must ensure full-thickness closure | Angle of needle guide between 10-20 degrees |
| Can clamp the trocar in place throughout the procedure | Ridges can withstand >15 lb force |
| Lightweight | Weighs less than 10 lbs |
| Easy to use | Adds less than 4 steps to current procedure |
Previous Prototypes
We have come a long way. Below are some of our earlier prototypes:
- The Trocar Cutter: A trocar that can cut through the layers of the abdominal wall to reduce the resistive force.
- The Trocar Spreader: A trocar that can manually spread the layers of the abdomen away to reduce the resistive force.
- The Trocar Puller: A device that can be deployed in the fat layer of the abdominal wall to pull the layers away from abdominal organs and create more space.
- The Trocar Stopper: A trocar accessory that serves as a thick external layer which stops the trocar from going farther into the abdomen than intended.
Some of the ideas were left behind based on negative voice of the customer feedback. Others were modified to be incorporated in the current design.




Surgeon Testimonials
“[Trocar insertion] is the most dangerous part of laparoscopic procedures”
Dr. Eva Galka, MD
“This! This is exactly what I have been asking for, for years”
Dr. Michael Aronis, MD
“Initially I didn’t see the value of your device, but now you are solving so many pains that occur in the OR”
Dr. Rabih Salloum, MD
Market Opportunity

- With $242,000 being the average cost of a settlement and a rate of major complications caused by laparoscopic access injuries ranging from 1.8 to 5.4 per 1,000 procedures, SafeT saves hospitals between $440 and $1,400 per surgery. Our cost-saving analysis and comparables analysis allow us to price the SafeT at $70 a unit.
- As our device is a first of its kind, we are creating a Niche market that grows in parallel with the trocar market (a subset of laparoscopic and robotic surgical device market). The more laparoscopic and robotic surgeries are performed, the greater the need for the SafeT device; the greater the success of the SafeT device in reducing complication rates, the more open surgeons would be to adopting more of such minimally invasive surgeries.
- The values of the minimally invasive devices ($16B) and trocar markets ($1B) are shown to the left. In addition, our expected addressable market based on our 5-year projection is also shown on the left ($33M)
Competitors

There are currently no devices on the market that successfully reduce the risk of organ or vessel puncture. LapCap, a device that is no longer on the market, is only compatible with Veress Needles and has shown no statistically significant data showing a reduction in the rate of complications. There are devices that allow for full-thickness closure and stabilize trocars during surgeries, but they add excessive costs and only work with a certain set of trocars. In addition, according to Voice of the Customer feedback, the current solutions to the wound site closure pain point are timely and can be difficult to use in some patients. That is because they can only be used after trocar insertion, at which point the initial incision path is no longer preserved. The SafeT device allows for wound site closure while the tissues are still separated, which our customers and advisors have said can save substantial time when closing the trocar wound site.
SafeT is the only device that can solve all three pain points. It is also expected to outperform all devices on the market in safety, efficacy, time, and cost-effectiveness. Finally, SafeT is trocar agnostic- it can be used with any trocar or method that the surgeon prefers.
Regulatory Strategy
Pre-Submission Meeting with the FDA to discuss regulatory strategy
Testing the final prototype: mechanical, chemical, and material testing
Submission of a De Novo classification request to the FDA
Testing
Will the adhesive stick to the skin?

A testing procedure (shown above) was developed to test whether or not the adhesive can withstand the 25 lb pulling force specified by our subject matter experts. The results of initial testing showed a maximum force of 25.52 lb, but our statistical analysis gave a p-value greater than 0.05 when comparing our test results with a target value of 25 lb. In order to ensure more confidence that the adhesive can withstand the pulling force, we have initiated contact with subject matter experts at 3M to find the optimal adhesive material for our application. In addition, we will be performing a DOE that tests the effects of different factors on the durability of the adhesive (such as attachment area, shape, and method of attachment)
Will the device break when pulled up with clamps?
A point force simulation was performed using Fusion 360 on the CAD model of the device. The model could withstand 15 times the specification for the pulling force. We plan on testing the final, printed model as well using the MTS tensile testing system.
Other Tests

There are several other aspects of the final product that will require testing. This testing is necessary to ensure that the device is safe and can effectively perform its role in reducing the rate of major complications in minimally-invasive surgeries. The figure above shows the mechanical considerations that have been tested or will be tested. In addition to these tests, it is important to perform Extractables and Leachables testing to ensure that no potentially harmful materials could harm patients during the use of the SafeT device. Finally, we plan on performing biocompatibility testing to ensure that the materials used in the device are safe to be in direct contact with the human body.
Our Team


